Part A: Informed Consent, Release Agreement, and Authorization
Full name: ___________________________________________
Date of birth: _________________________________________
A
High-adventure base participants:
Expedition/crew No.: _______________________________________________
or staff position: ___________________________________________________
680-001
2019 Printing
Adults NOT Authorized to Take Youth to and From Events:
Informed Consent, Release Agreement, and Authorization
I understand that participation in Scouting activities involves the risk of personal injury, including
death, due to the physical, mental, and emotional challenges in the activities offered. Information
about those activities may be obtained from the venue, activity coordinators, or your local council.
I also understand that participation in these activities is entirely voluntary and requires participants
to follow instructions and abide by all applicable rules and the standards of conduct.
In case of an emergency involving me or my child, I understand that efforts will be made to
contact the individual listed as the emergency contact person by the medical provider and/or
adult leader. In the event that this person cannot be reached, permission is hereby given to the
medical provider selected by the adult leader in charge to secure proper treatment, including
hospitalization, anesthesia, surgery, or injections of medication for me or my child. Medical
providers are authorized to disclose protected health information to the adult in charge, camp
medical staff, camp management, and/or any physician or health-care provider involved in
providing medical care to the participant. Protected Health Information/Condential Health
Information (PHI/CHI) under the Standards for Privacy of Individually Identiable Health Information,
45 C.F.R. §§160.103, 164.501, etc. seq., as amended from time to time, includes examination
ndings, test results, and treatment provided for purposes of medical evaluation of the participant,
follow-up and communication with the participant’s parents or guardian, and/or determination of
the participant’s ability to continue in the program activities.
(If applicable) I have carefully considered the risk involved and hereby give my informed consent
for my child to participate in all activities offered in the program. I further authorize the sharing
of the information on this form with any BSA volunteers or professionals who need to know of
medical conditions that may require special consideration in conducting Scouting activities.
With appreciation of the dangers and risks associated with programs and activities, on my
own behalf and/or on behalf of my child, I hereby fully and completely release and waive
any and all claims for personal injury, death, or loss that may arise against the Boy Scouts
of America, the local council, the activity coordinators, and all employees, volunteers,
related parties, or other organizations associated with any program or activity.
I also hereby assign and grant to the local council and the Boy Scouts of America, as well as their
authorized representatives, the right and permission to use and publish the photographs/lm/
videotapes/electronic representations and/or sound recordings made of me or my child at all
Scouting activities, and I hereby release the Boy Scouts of America, the local council, the activity
coordinators, and all employees, volunteers, related parties, or other organizations associated
with the activity from any and all liability from such use and publication. I further authorize the
reproduction, sale, copyright, exhibit, broadcast, electronic storage, and/or distribution of said
photographs/lm/videotapes/electronic representations and/or sound recordings without limitation
at the discretion of the BSA, and I specically waive any right to any compensation I may have for
any of the foregoing.
Every person who furnishes any BB device to any minor, without the express or implied permission
of the parent or legal guardian of the minor, is guilty of a misdemeanor. (California Penal Code
Section 19915[a]) My signature below on this form indicates my permission.
I give permission for my child to use a BB device. (Note: Not all events will include BB devices.)
Checking this box indicates you DO NOT want your child to use a BB device.
List participant restrictions, if any: None
________________________________________________________
Complete this section for youth participants only:
Adults Authorized to Take Youth to and From Events:
You must designate at least one adult. Please include a phone number.
Name: _________________________________________________________________
Phone: _________________________________________________________________
Name: _________________________________________________________________
Phone: _________________________________________________________________
Name: _________________________________________________________________
Phone: _________________________________________________________________
Name: _________________________________________________________________
Phone: _________________________________________________________________
I understand that, if any information I/we have provided is found to be inaccurate, it may limit and/or eliminate the opportunity for participation in any event or activity. If I am participating at
Philmont Scout Ranch, Philmont Training Center, Northern Tier, Sea Base, or the Summit Bechtel Reserve, I have also read and understand the supplemental risk advisories, including height
and weight requirements and restrictions, and understand that the participant will not be allowed to participate in applicable high-adventure programs if those requirements are not
met. The participant has permission to engage in all high-adventure activities described, except as specically noted by me or the health-care provider. If the participant is under the age of 18, a
parent or guardian’s signature is required.
Participant’s signature: ____________________________________________________________________________________________ Date: ______________________________
Parent/guardian signature for youth: __________________________________________________________________________________ Date: ______________________________
(If participant is under the age of 18)
NOTE: Due to the nature of programs and activities, the Boy Scouts of
America and local councils cannot continually monitor compliance of program
participants or any limitations imposed upon them by parents or medical
providers. However, so that leaders can be as familiar as possible with any
limitations, list any restrictions imposed on a child participant in connection with
programs or activities below.
Part B1: General Information/Health History
Full name: ___________________________________________
Date of birth: _________________________________________
B1
High-adventure base participants:
Expedition/crew No.: _______________________________________________
or staff position: ___________________________________________________
In case of emergency, notify the person below:
Name: ______________________________________________________________________________Relationship: ___________________________________________________
Address: _________________________________________________________________ Home phone: _________________________ Other phone: _________________________
Alternate contact name: _________________________________________________________________ Alternate’s phone: ______________________________________________
Age: ____________________________ Gender: __________________________ Height (inches): ___________________________ Weight (lbs.): ____________________________
Address: _________________________________________________________________________________________________________________________________________
City: ___________________________________________State: ____________________________ ZIP code: __________________ Phone: ______________________________
Unit leader: ____________________________________________________________________________ Unit leader’s mobile #: _________________________________________
Council Name/No.: _______________________________________________________________________________________________________Unit No.: ____________________
Health/Accident Insurance Company: ________________________________________________________ Policy No.: ___________________________________________________
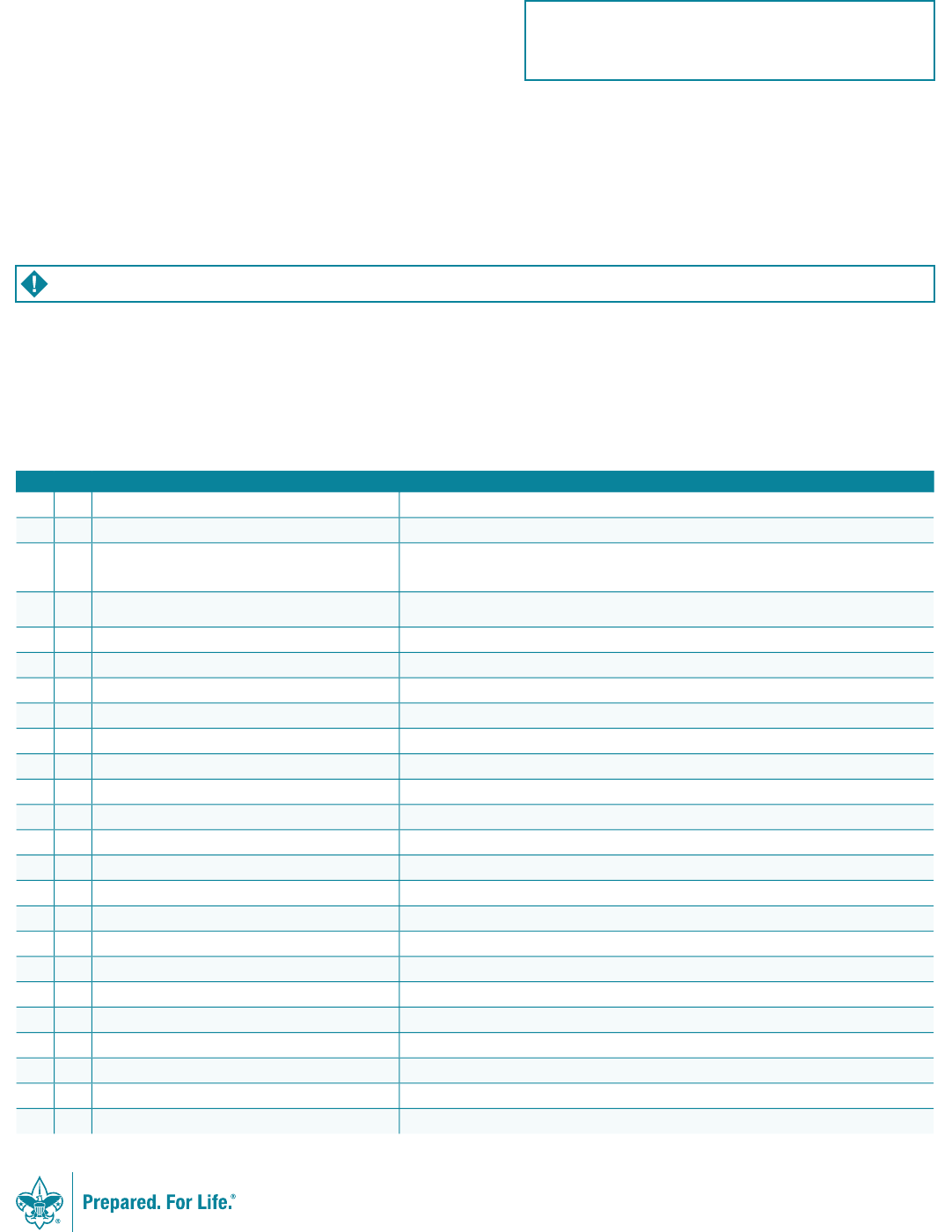
Health History
Do you currently have or have you ever been treated for any of the following?
Yes No Condition Explain
Diabetes
Last HbA1c percentage and date: Insulin pump: Yes £ No £
Hypertension (high blood pressure)
Adult or congenital heart disease/heart attack/chest pain (angina)/
heart murmur/coronary artery disease. Any heart surgery or
procedure. Explain all “yes” answers.
Family history of heart disease or any sudden heart-related
death of a family member before age 50.
Stroke/TIA
Asthma/reactive airway disease
Last attack date:
Lung/respiratory disease
COPD
Ear/eyes/nose/sinus problems
Muscular/skeletal condition/muscle or bone issues
Head injury/concussion/TBI
Altitude sickness
Psychiatric/psychological or emotional difculties
Neurological/behavioral disorders
Blood disorders/sickle cell disease
Fainting spells and dizziness
Kidney disease
Seizures or epilepsy
Last seizure date:
Abdominal/stomach/digestive problems
Thyroid disease
Skin issues
Obstructive sleep apnea/sleep disorders
CPAP: Yes £ No £
List all surgeries and hospitalizations
Last surgery date:
List any other medical conditions not covered above
680-001
2019 Printing
Please attach a photocopy of both sides of the insurance card. If you do not have medical insurance, enter “none” above.
Part B2: General Information/Health History
Full name: ___________________________________________
Date of birth: _________________________________________
B2
High-adventure base participants:
Expedition/crew No.: _______________________________________________
or staff position: ___________________________________________________
YES NO Non-prescription medication administration is authorized with these exceptions: ________________________________________________________________
Administration of the above medications is approved for youth by:
_______________________________________________________________________ / _______________________________________________________________________
Parent/guardian signature MD/DO, NP, or PA signature (if your state requires signature)
Please list any additional information about your
medical history:
_________________________________________
_________________________________________
_________________________________________
_________________________________________
DO NOT WRITE IN THIS BOX.
Review for camp or special activity.
Reviewed by: ___________________________________________
Date: _________________________________________________
Further approval required:
Yes No
Reason: _______________________________________________
Approved by: ____________________________________________
Date: _________________________________________________
DO YOU USE AN EPINEPHRINE YES NO
AUTOINJECTOR? Exp. date (if yes) ___________________________
DO YOU USE AN ASTHMA RESCUE YES NO
INHALER? Exp. date (if yes) ___________________________________
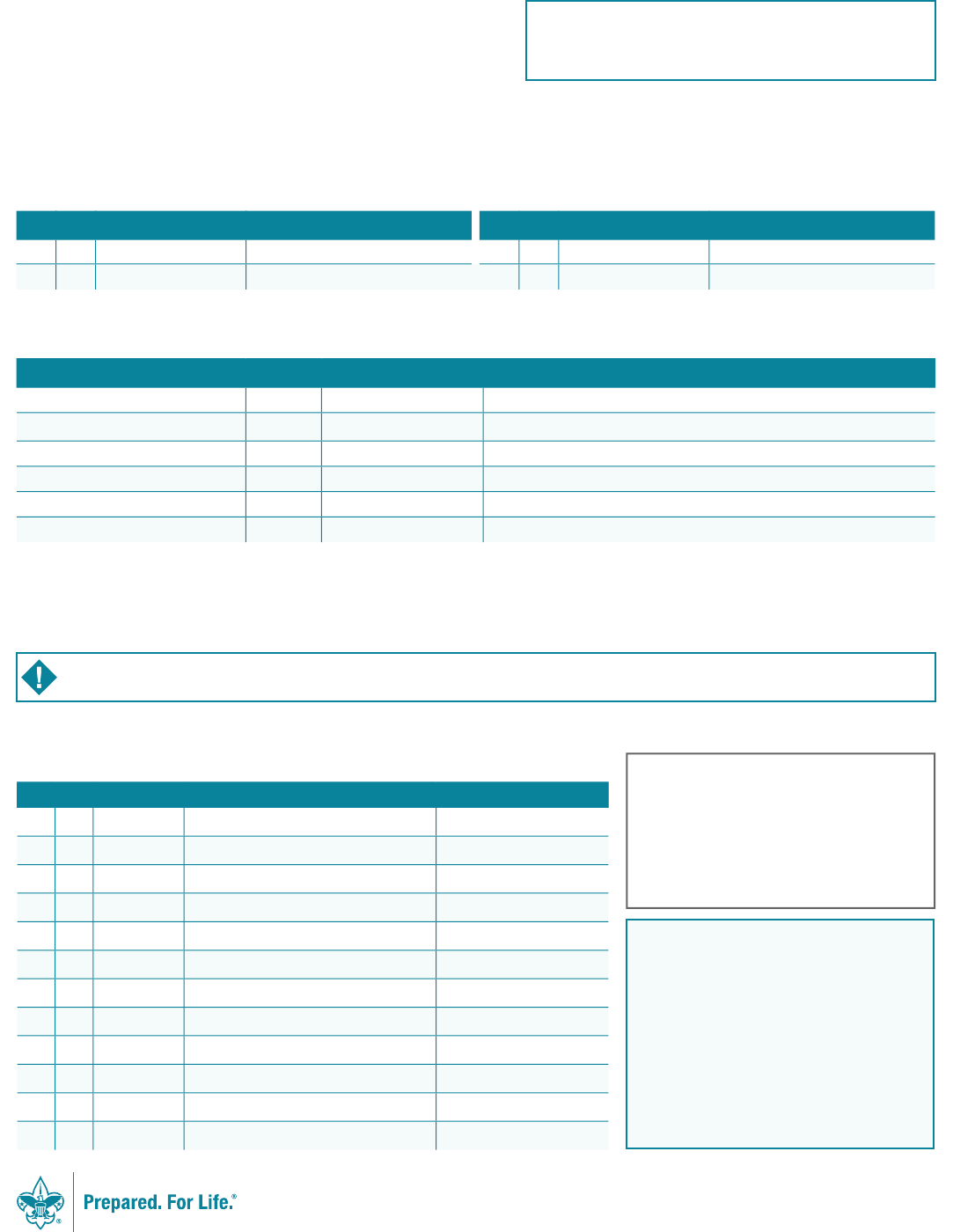
Allergies/Medications
Immunization
Are you allergic to or do you have any adverse reaction to any of the following?
Yes No Allergies or Reactions Explain Yes No Allergies or Reactions Explain
Medication Plants
Food Insect bites/stings
List all medications currently used, including any over-the-counter medications.
Check here if no medications are routinely taken. If additional space is needed, please list on a separate sheet and attach.
Medication Dose Frequency Reason
The following immunizations are recommended. Tetanus immunization is required and must have been received within the last 10
years. If you had the disease, check the disease column and list the date. If immunized, check yes and provide the year received.
Yes No Had Disease Immunization Date(s)
Tetanus
Pertussis
Diphtheria
Measles/mumps/rubella
Polio
Chicken Pox
Hepatitis A
Hepatitis B
Meningitis
Inuenza
Other (i.e., HIB)
Exemption to immunizations (form required)
680-001
2019 Printing
Bring enough medications in sufcient quantities and in the original containers. Make sure that they are NOT expired, including inhalers and EpiPens. You SHOULD NOT STOP taking
any maintenance medication unless instructed to do so by your doctor.
Part C: Pre-Participation Physical
This part must be completed by certied and licensed physicians (MD, DO), nurse practitioners, or physician assistants.
Full name: ___________________________________________
Date of birth: _________________________________________
C
High-adventure base participants:
Expedition/crew No.: _______________________________________________
or staff position: ___________________________________________________
Please ll in the following information:
Yes No Explain
Medical restrictions to participate
Height/Weight Restrictions
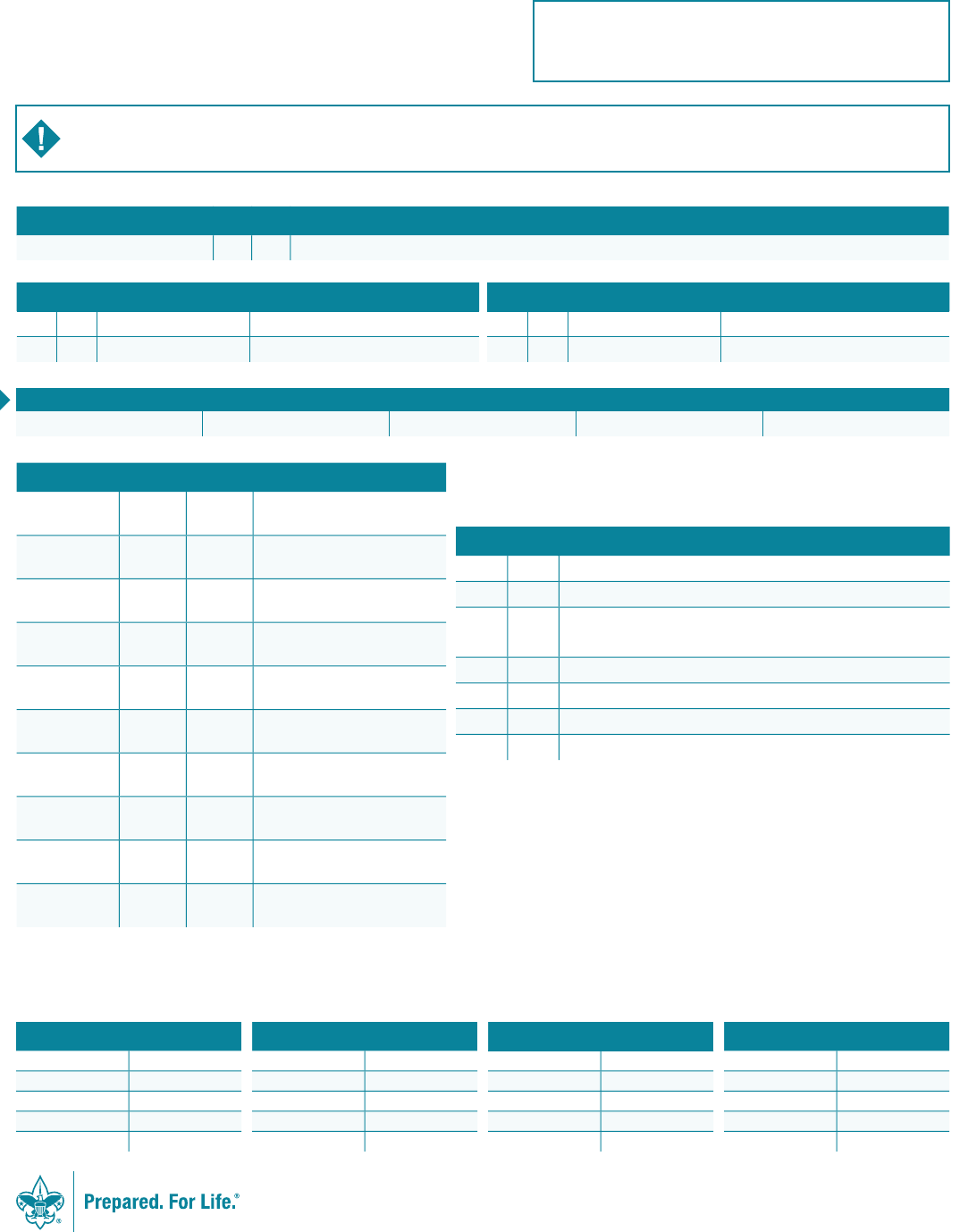
If you exceed the maximum weight for height as explained in the following chart and your planned high-adventure activity will take you more than 30 minutes away from an emergency vehicle/
accessible roadway, you may not be allowed to participate.
Maximum weight for height:
Height (inches) Max. Weight Height (inches) Max. Weight Height (inches) Max. Weight Height (inches) Max. Weight
60 166 65 195 70 226 75 260
61 172 66 201 71 233 76 267
62 178 67 207 72 239 77 274
63 183 68 214 73 246 78 281
64 189 69 220 74 252 79 and over 295
Examiner’s Certication
I certify that I have reviewed the health history and examined this person and nd no contraindications for
participation in a Scouting experience. This participant (with noted restrictions):
True False Explain
Meets height/weight requirements.
Has no uncontrolled heart disease, lung disease, or hypertension.
Has not had an orthopedic injury, musculoskeletal problems, or orthopedic
surgery in the last six months or possesses a letter of clearance from his or her
orthopedic surgeon or treating physician.
Has no uncontrolled psychiatric disorders.
Has had no seizures in the last year.
Does not have poorly controlled diabetes.
If planning to scuba dive, does not have diabetes, asthma, or seizures.
Examiner’s signature: _______________________________________ Date: _______________
Examiner’s printed name: _________________________________________________________
Address: _______________________________________________________________________
City: ______________________________________State: ______________ ZIP code: _________
Ofce phone: ___________________________________________________
Normal Abnormal Explain Abnormalities
Eyes
Ears/nose/throat
Lungs
Heart
Abdomen
Genitalia/hernia
Musculoskeletal
Neurological
Skin issues
Other
Yes No Allergies or Reactions Explain Yes No Allergies or Reactions Explain
Medication Plants
Food Insect bites/stings
680-001
2019 Printing
Height (inches) Weight (lbs.) BMI Blood Pressure Pulse
/
You are being asked to certify that this individual has no contraindication for participation in a Scouting experience. For individuals who will be attending a high-adventure program,
including one of the national high-adventure bases, please refer to the supplemental information on the following pages or the form provided by your patient. You can also visit
www.scouting.org/health-and-safety/ahmr to view this information online.

680-001
October 2019
Northern Tier Experience. Participation at any of the BSA’s
high-adventure bases or in any unit high-adventure backcountry/wilderness
activities can be physically, mentally, and emotionally demanding. Each high-
adventure base offers a unique experience that is not risk-free. Knowledgeable
staff will instruct all participants in safety measures to be followed. Be
prepared to listen to and carefully follow these safety measures and to accept
responsibility for the health and safety of yourself and others.
Northern Tier Requirements. Each person must be able
to carry a 50- to 85-pound pack or canoe from a quarter-mile to 2 miles several
times a day on rough, swampy, and rocky portages and paddle 10 to 15 miles per
day, often against a headwind. The portage trails can be very muddy, slippery,
and rocky, and those conditions can potentially lead to tripping and falling. All
participants must wear boots that cover their ankles while on the trails. Climatic
conditions can range from 30 to 100 degrees in summer/autumn and from –40
to 40 degrees in the winter. During the Okpik Experience, each person will walk,
ski, or snowshoe along snow-covered trails or across frozen lakes, pulling loaded
toboggans or sleds for up to 3 miles—or more if on a cross-country ski trek.
Refer to the Northern Tier website for specific information.
Be Prepared. While participating in Northern Tier’s canoeing and
camping backcountry/wilderness areas, life jackets must be worn at all times
when on the water. Crew members travel together at all times. Emergency
communications via radio, and in more remote locations by satellite phone, are
provided by Northern Tier. Radio communication and/or emergency evacuation
can be hampered by weather, terrain, distance, time of day, equipment
malfunction, and other factors, and are not a substitute for taking appropriate
precautions and having adequate first-aid knowledge and equipment. Please
call Northern Tier at 218-365-4811 if you have any questions.
Seizures (Epilepsy). The seizure disorder must be well-
controlled by medication. A well-controlled disorder is one in which a year has
passed without a seizure. Exceptions to this guideline may be considered on an
individual basis and will be based on the specific type of seizure and likely risks
to the individual and/or other members of the crew.
Diabetes Mellitus. Both the person with diabetes and one
other person in the group need to be able to recognize signs of excessively
high or low blood sugar and adjust the dose of insulin. An insulin-dependent
person who was diagnosed or who has had a change in delivery system (e.g.,
insulin pump) in the last six months is advised not to participate. A person with
diabetes who has had frequent hospitalizations or who has had problems with
low blood sugar should not participate until better control of the diabetes has
been achieved.
Asthma. Asthma must be well-controlled before participating. This
means: 1) the use of a rescue inhaler (albuterol) less than two times per week
(except use for the prevention of exercise-induced asthma); 2) nighttime
awakenings for asthma symptoms less than two times per month. Well-
controlled asthma may include the use of long-acting bronchodilators, inhaled
steroids, or oral medications such as Singulair. You may not be allowed to
participate if: 1) you have asthma not controlled by medication; or 2) you have
been hospitalized/gone to the emergency room to treat asthma in the past
six months; or 3) you have needed treatment by oral steroids (prednisone) in
the past six months. You must bring an ample supply of your medication and
a spare rescue inhaler that are not expired. At least one other member of the
crew should know how to use the rescue inhaler. Any person who has needed
treatment for asthma in the past three years must carry a rescue inhaler on the
trek. If you do not bring a rescue inhaler, you must buy one before you will be
allowed to participate.
Allergy or Anaphylaxis. People who have had an
anaphylactic reaction from any cause will be required to keep appropriate
treatment including epinephrine with them. You and at least one other member
of your crew must know how to give the treatment. If you do not bring
appropriate treatment with you, you will be required to buy it before you will be
allowed to participate.
Recent Musculoskeletal Injuries and
Orthopedic Surgery. Participants will put a great deal of strain
on their joints. Individuals who have significant musculoskeletal problems
(including back problems) or have had orthopedic surgery or injuries within the
last six months must have a letter of clearance from their treating physician to
be considered for approval, and Northern Tier should be contacted in advance
of participation. Permission is not guaranteed.
Psychological and Emotional Difficulties.
Parents and advisors should be aware that no high-adventure experience
is designed to assist participants in overcoming psychological or emotional
problems. Experience demonstrates that these problems frequently become
worse when a participant is under stress from the physical and mental
challenges of a remote wilderness setting. Medication must never be stopped
prior to participation and should be continued throughout the entire experience.
Cardiac or Cardiovascular Disease. Adults or youth
who have a history of chest pain, myocardial infarction (heart attack), a family
history of premature heart disease, or heart surgery including angioplasty may
consider a physician-supervised stress test. Even if the stress test results
are normal, the testing is done without portage packs or canoes and does not
guarantee safety. If the results are abnormal, the individual is advised not
to participate.
Medication. Each participant who needs medication must bring
enough medication for the duration of the trip, as well as enough to store
two supplies in two separate locations. Due to the possibility of packs and
equipment getting wet, every attempt is made to store medications in two
separate packs in different canoes while traveling.
Weight Limits. Each participant in a Northern Tier expedition should
not exceed the maximum acceptable weight for height in the table shown in
Part C of the Annual Health and Medical Record. Those who fall within the
recommended weight limits are much more likely to have an enjoyable trek and
avoid incurring injuries and other health risks. Due to the risks of logistics of
backcountry rescue, no participant’s weight can exceed 295 pounds.
Phone: 218-365-4811 Website: www.ntier.org
High-Adventure Risk Advisory to
Health-Care Providers and Parents
Northern Tier
